

By Mary Lee
Ocean-themed décor splashes the walls of La Rabida Children’s Hospital in a room filled with bright, plush chairs contoured like the candy Dots. But perky colors can’t erase the worry on Maria Gallegos’ face as she sits in the room waiting for her 6-year-old daughter to finish her appointment.
She’s lost count of the routine check-ups after dipping in and out of hospitals since her daughter’s conception. Born seven weeks premature, Lindsey championed through multiple surgeries including a tracheostomy, which helped her breathe; and a gastrostromy (G-Tube), which channeled nutrients through her body via an inserted tube. At eight months old, Lindsey and her twin Mackenzie were diagnosed with Achondroplasia dwarfism, a form of short-limbed dwarfism.



Gallegos’ curly brown hair was pulled back in a ponytail as she quietly sat next to her 3-year-old daughter. Natural light saturated the room through the floor-to-ceiling windows facing a shoreline view of blue, speckled with large chunks of ice bobbing in Lake Michigan.
For six years, she visited multiple hospitals around Chicago to treat the twins’ conditions. When they were born, she had only lived in Chicago for a year since emigrating from Mexico. Her limited English impeded her understanding of why doctors told her to switch hospitals on numerous occasions, she said. They had directed Lindsey to the University of Chicago Medicine, while sending Mackenzie to the University of Illinois at Chicago Medical Center.
“Usually, when they told me to see a new doctor, it was awful because the new doctor didn’t have the documentation,” she said. If patients move hospitals, medical records need to be forwarded to the new hospital. And these medical record transfers delayed for up to four weeks, she explained.
When proper documentation and medical records weren’t sent to the appropriate hospital in a timely manner, she had to reschedule her daughter’s appointments. If there was an emergency, she had no choice but to take Lindsey to the emergency room.
Lindsey’s story is a common one.
Introducing electronic health records
The U.S. government addressed this problem by incentivizing adoption of electronic health records (EHRs) to replace paper-based records. This mandate granted both patients and health care providers access to medical history, medication, health history, images, laboratory test results and more. Its major incentive: to make health care more efficient.
Cue the private sector.
The private sphere, home to EHR systems, developed into a competitive bloodbath, in which many startup companies hopped aboard to innovate and address disparities in health care efficiency. Chicago has pulsated into a hotbed for the latest health care startup contenders- many promoting efficiency as their ticket to playing with the big boys.
In the past, physicians handwrote all notes, lab orders, medication history and relevant information pertaining to a patient’s health history. The papers amassed in manila folders were maintained at each separate hospital. For Gallegos, this was one aggravating reason why it took so long for physical documents to be transferred to other hospitals. But technological advancements have unspooled the musty layers of this outdated system, unbridling a cornucopia of endless possibilities to advance health care.
“Nobody wants to go back to paper charts,” said Dr. Stan Sonu, a physician at Rush University Medical Center. “Nobody. It’s an archaic method.”
EHRs facilitate, collect, store and share comprehensive information for health care providers to help them make informed decisions. The comprehensive archive of information helps providers make the appropriate diagnosis and lowers chances for medical errors.
Information technology accounts for as much as one-third of hospitals’ capital spending, according to a study published September 2014 by the Office of the National Coordinator for Health Information Technology (ONC).
The Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009 enacted a federal adoption of an electronic use and exchange of health information.
What are electronic health records?
There are two types of EHRs: a basic EHR and a comprehensive EHR. The basic EHR reports full implementation of 10 computerized functions in at least one clinical unit of the hospital including electronic maintenance of patient information, notes, assessments, medication lists, discharges, summaries, laboratory reports, diagnostic test results, and electronic ordering of medication.
A comprehensive EHR performs all functions of the basic model but includes 14 additional functions, which are performed and implemented in all major clinical units.
La Rabida Children’s Hospital implemented the EHR system MEDITECH in 2011, and is one stage shy of being entirely paper-less.
“To be considered an advanced well-run hospital, you pretty much have to have an electronic medical record system. In some ways, you can think of it as the price of admission for doing business in the health care field right now,” said Robert Chess, a lecturer at Stanford University’s Graduate School of Business and chairman of Nektar Therapeutics.
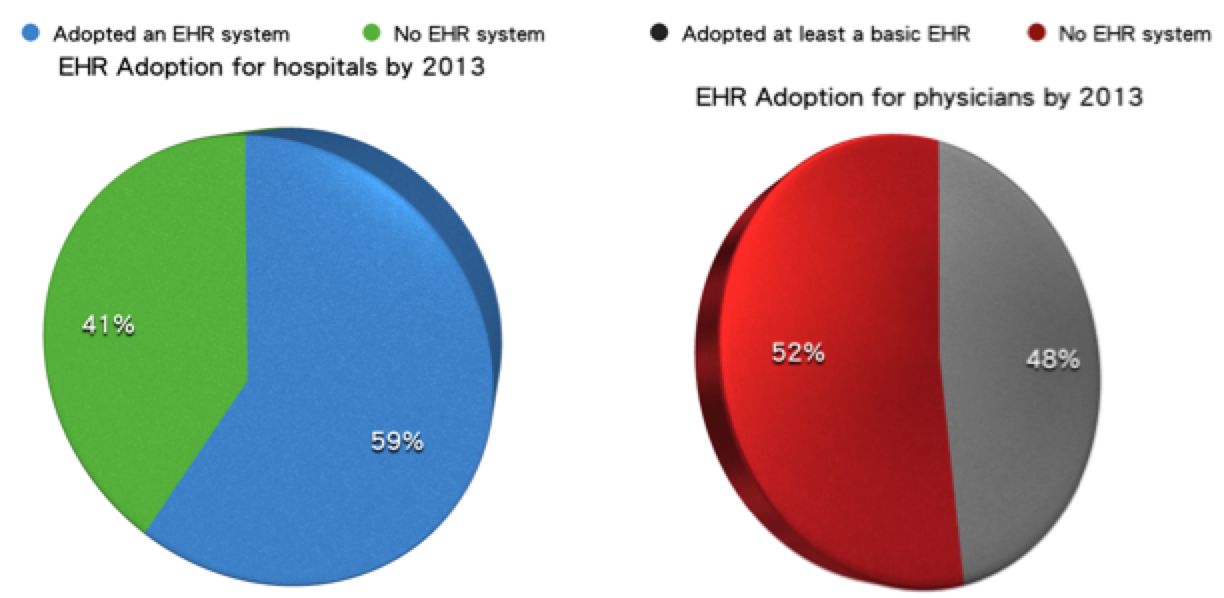
At the end of 2013, nearly 60 percent of hospitals adopted a basic or comprehensive EHR, quadruple the statistic in 2010, and 48 percent of physicians had at least a basic EHR system, according to an October 2014 report to Congress on Health IT Adoption and HIE.
Although the rate of acceptance and use increased fourfold after 2010, “it’s still been very difficult with independent physician practices because you need a certain level of infrastructure there. And the economies of scale don’t necessarily support adoption by small practices,” explained Dr. Rishi Agrawal, a physician at La Rabida Children’s Hospital and Lurie Children’s Hospital.
Critical-access hospitals, which mainly serve rural populations, and individual practicing physicians, straggled behind, according to the ONC. Data indicated that medium-sized hospitals are increasingly gaining momentum because of increased purchasing power and resources to implement EHRs.
The problem with EHRs: incompatibility, high costs and implementation
Although the competitive market touts EHRs handy customized functionalities, its extreme technicalities have ultimately inhibited interoperability and stifled its goal of a streamlined transfer of information amongst providers.
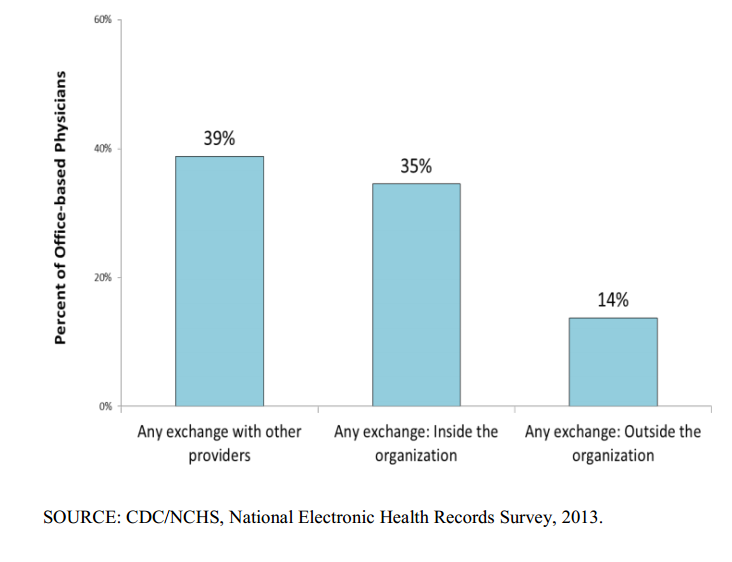
EHRs were intended to take information out of silos, abandon paper charts, and streamline data; however, without interoperability, the promise remains unrealized. A majority of physicians have not engaged in information exchange outside of their organization because two different platforms are often not compatible, according to the Centers for Disease Control and Prevention (CDC) and National Center for Health Statistics (NCHS) data brief.
“All of their products don’t talk to each other,” said David Dranove, a Northwestern University professor at the Kellogg School of Management and health care expert in industrial organization and business strategy. Imagine a situation where you’re trying to use your Verizon phone in an area where only AT&T has cellular service. There might be two cell phones, but you won’t be able to talk to each other.
Only 14 percent of physicians shared electronic health information outside their organization because of interoperability issues. The private sector customizes different EHR platforms, which establishes inconsistent technical and medical vocabulary, structure and format.
“Frankly, the fact that records are not as interoperable as they should,” said Agrawal, “is probably a result of deliberate decisions by the electronic health record vendors who it’s not necessarily in their interest to make them work very well with each other because their business models are predicated on selling more licenses of their product.”
An incentive to adopt EHRs was to save a projected trillion dollars in health care costs. However, the hefty price tag has not quite offset its presumed benefits. Depending on the size of the system, number of patients and providers, and a variety of other factors, a system could cost upwards of several hundred million dollars.
“It’s more promise than fulfillment,” Dranove said. Lack of technology education, EHR implementation and lack of interoperability only exacerbate already high costs in purchasing EHR implementation.
And the road to logistically adopting these systems is not easy. Implementation chews up most of the cost.
“They’re not all user friendly, they’re not all intuitive,” Sonu commented regarding the EPIC EHR system at Rush hospital. “I’m not a programmer, but it seems like it was built off of Windows 95- an old PC platform.”
Generation gaps between seasoned doctors accustomed to the old model of health records and younger tech-savvy generation of doctors made EHR implementation difficult.
“Until five to 10 years ago, it was all with paper,” Sonu chuckled. “So, to get a 60-year-old doctor to start typing notes and typing orders, it’s hilarious to watch,” he said. “They’re seriously index fingering when typing in their names and log in. It takes them longer to navigate an EMR than paper charts.”
However, most doctors agree it’s time for a change. So does Gallegos.
“It’s easier because a year ago, La Rabida Hospital put information about the twins’ birth, how many times they checked in, their history and all the documentation in the computer,” Gallegos said. They also gave her a USB containing information to make it easier for other doctors to access all the documentation if she needed to go to a different hospital.
Huge potential in health care technology
With patients reaping tangible benefits from electronic records, Chicago’s investors, entrepreneurs and innovators are finding health care technologies an untapped gold mine.
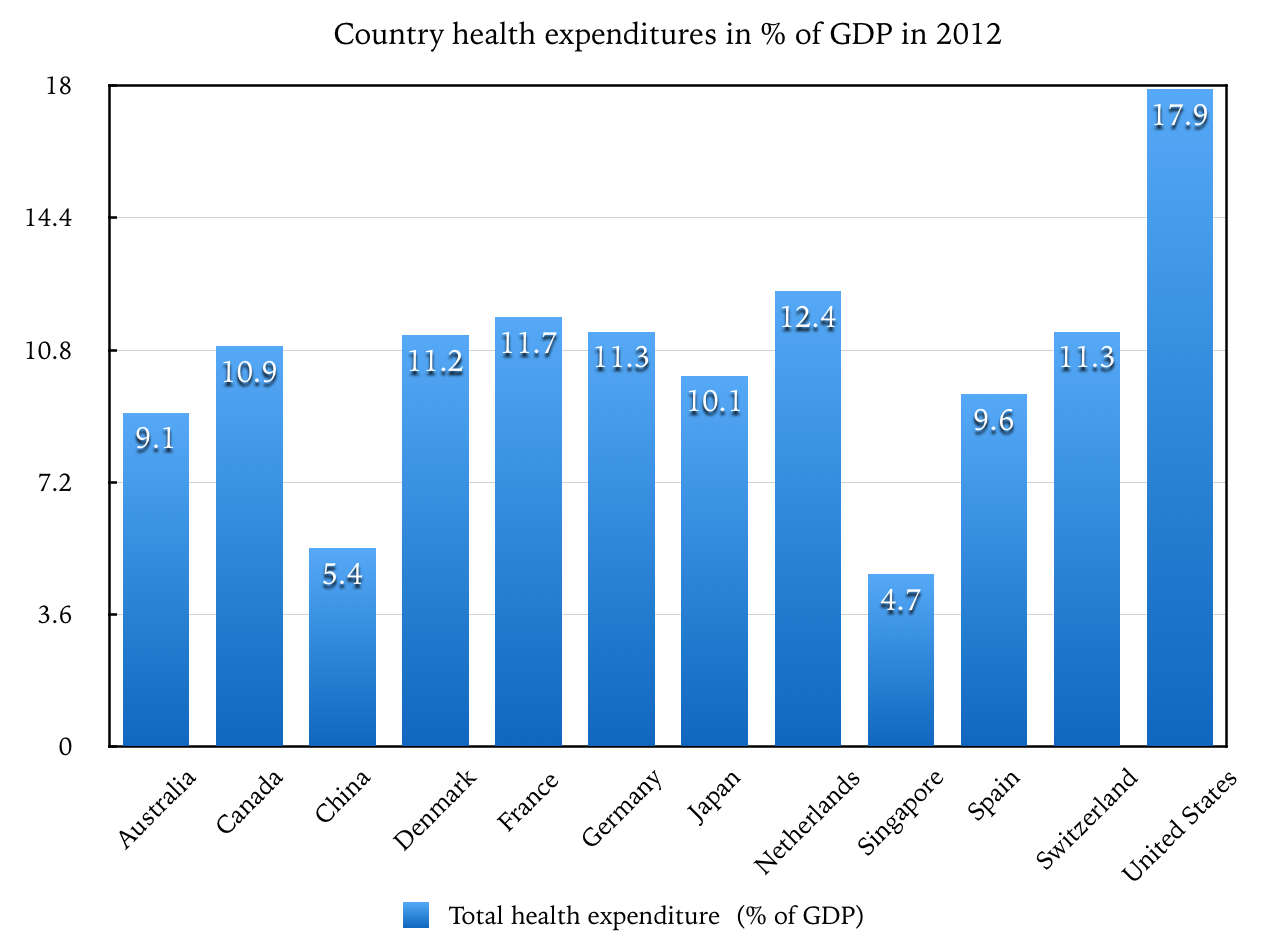
The United States spends 17 percent of GDP on health care, about $2.9 trillion a year, Chess said. In comparison to other developed countries, U.S. numbers surpassed by about 6 percent.
“Entrepreneurs look at that and say that’s a huge opportunity,” Chess said.
For Steve Sprieser, co-founder of the start-up company Varsa Health, he created a measurement tool for behavior health- a platform to advance patient treatments and research by standardizing a vehicle to capture patient outcomes.
“Behavioral health has by and large lagged when it comes to being able to capture patient outcomes in any sort of electronic form,” Sprieser said. “It has been paper-based. It has not been standardized.”
Varsa Health enables consumers to provide an iterative feedback loop to their clinicians beyond the four walls of their provider or clinical setting via smart phone applications, text messaging and other wearables individuals may use to monitor their own health. The collected information is then available to his or her clinician or case manager to better fine-tune treatments through the recovery process.
The company seeks a holistic approach by integrating mental health and behavioral health into care, said Miraj Chokshi, Varsa Health co-founder. “Technology is really going to be the way to move towards this.”
Though the innovation fresh startup companies bring to the table are applaudable, there are concerns whether these technologies and products can co-exist.
“Hospitals are being inundated by so many different information systems,” Chess said. “It makes it hard for startups to get noticed because hospitals have all these EMR systems that they’re putting in.” However, the determining factor for a successful startup is a strong economic rationale for hospitals or providers to adopt their product, Chess explained.
Chicago startup investments and exits surged in 2014, with more than 150 companies raising $1.6 billion in capital and 34 companies exiting for more than $7 billion, according to a Chicago startup report by Built in Chicago.
“The great tension that you have between small startup innovators that come up with great new ideas for using technology, and trying to integrate those existing platforms” would be a challenge to integrate those innovations into mainstream practice, Dranove said.
Sprieser acknowledged the need for technology that can operate on different systems. “So for us, it’s being able to work with the existing technologies, that’s out there such as EHRs,” he said acknowledging the existing competitive market. But, he also added the need for advancing patient care by enabling other forms of technology, such as activity trackers, sensors and metric data.
The market solution will take time. Eventually, providers will gravitate towards a software product with uniform interoperability.
Many startups and earlier versions of EHRs flopped because it was a new market, Dr. Agrawal said. “Some of those folks are being shaken out of the market. And the more established providers are succeeding.”
Good news for consumers is that once these technology snags uncoil, there could be lower health care costs. When there have been cost savings, Dranove said, “those savings have been passed along through to the insurers and onto the consumers. So, if providers realize savings, we as consumers will get the benefits. No question about that.”
The competitive market proves to be an arduous landscape for startups to find their unique niche and notarize their originality.
But if these innovative products have patient care at the fulcrum of their model, 6-year-old Lindsey could precipitously benefit from interoperable EHR systems and other health care technologies.
Apart from EHR, there are still many ways technology hasn’t broken into the behemoth-like health industry.
“Pagers, we have pagers still,” Sonu said incredulously. “I mean my pager is probably from the mid-1990s. Can’t there be a better system that’s developed to notify a doctor?”
